

Excessive eye watering without crying, called epiphora, is usually caused by one of two problems: your eyes are producing too many tears, or your tears cannot drain properly. Common triggers include dry eye syndrome, allergies, blocked tear ducts, wind exposure, and eye infections. Identifying the specific cause is the first step toward effective treatment.
Your eyes are soaking through tissues, blurring your vision mid-conversation, and yet you feel completely fine emotionally. It’s one of those symptoms that feels embarrassingly hard to explain. The truth is, persistent watery eyes are a real clinical condition with specific, treatable causes. Understanding what’s actually happening in your tear system changes everything about how you approach the problem.
Key Takeaways
- Excessive tearing (epiphora) is either caused by overproduction of tears or a failure in tear drainage, and the two require different treatments.
- Dry eye is one of the most counterintuitive culprits: when eyes become too dry, the brain triggers a reflex tear flood as a defense mechanism.
- Blocked tear ducts, allergies, eyelid problems, and environmental irritants are all distinct causes that each have specific management strategies.
- Watery eyes that persist for more than a few weeks, affect vision, or come with pain, discharge, or light sensitivity warrant a professional eye exam.
- Many cases of chronic epiphora are highly treatable once the underlying cause is accurately diagnosed.

What Is Epiphora and Why Does It Happen?
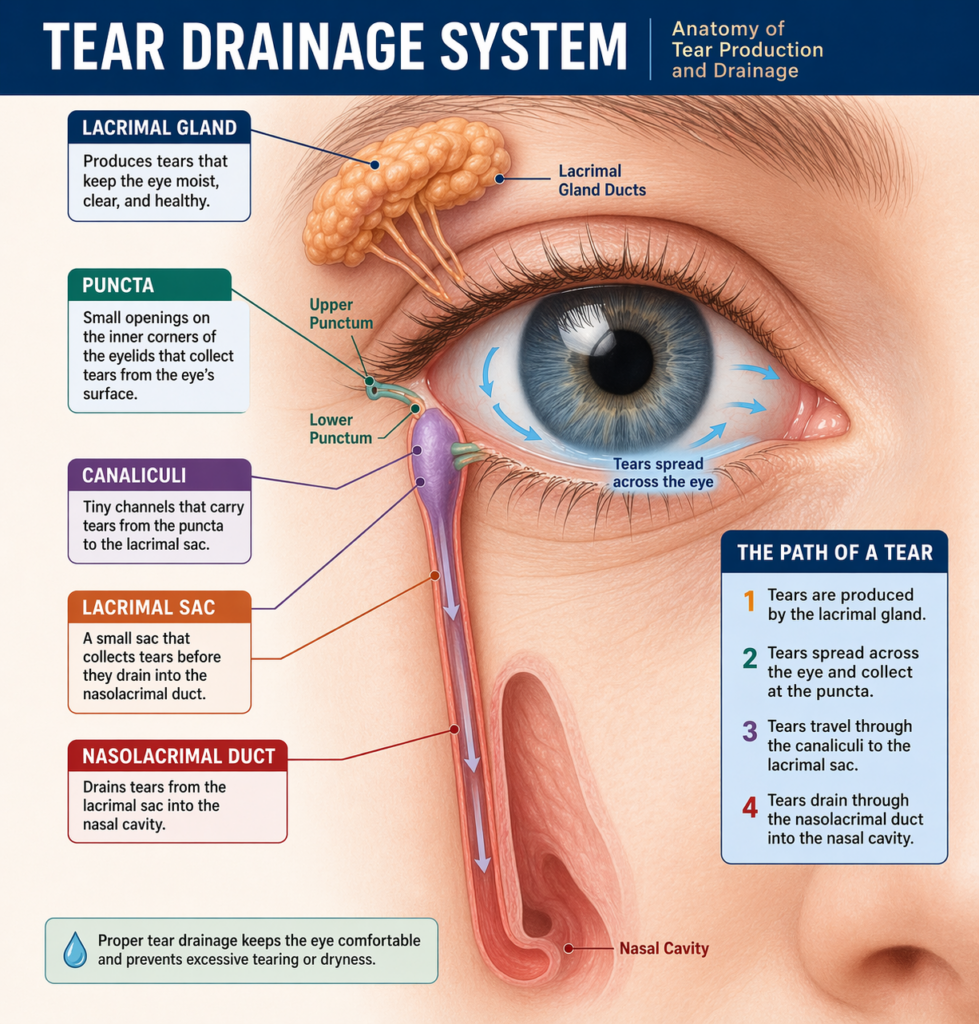
The medical term for excessive, involuntary tearing is epiphora. Your eyes produce tears constantly as part of normal function, they lubricate the surface, wash away debris, and protect against infection. Normally, tears drain through small openings called puncta at the inner corner of each eyelid, travel through the nasolacrimal duct, and empty into the nasal cavity.
When this system gets disrupted, tears spill over the eyelid margin instead of draining away. The disruption is almost always one of two things: your lacrimal gland is producing tears faster than the drainage system can handle, or the drainage pathway itself is blocked or narrowed. Both result in the same visible symptom, but they need to be treated very differently.
The Dry Eye Paradox: Why Dryness Causes Watering
This is the most misunderstood cause of excessive tearing, and it catches nearly everyone off guard. When the surface of your eye becomes chronically dry, sensory nerves send an emergency signal to the lacrimal gland, which responds by releasing a sudden flood of reflex tears. These reflex tears are a biological alarm response, not the steady, lubricating tears your eye actually needs.
The cruel irony is that reflex tears are mostly water. They lack the oils and mucin that make tears stick to the eye surface and provide real lubrication. So they overflow immediately, causing your eyes to stream, but the underlying dryness remains unchanged. This is why treating watery eyes with dry eye therapy, specifically lipid-based artificial tears or warm compresses, often resolves the tearing entirely.
Dry eye disease affects an estimated 16 million adults in the United States, and a significant proportion of those patients present with watery eyes rather than the dryness or burning sensation most people associate with the condition. This makes it one of the most frequently misdiagnosed causes of epiphora in clinical eye care settings.
Common Causes of Excessive Tearing at a Glance
| Cause | How It Triggers Tearing | Key Clue |
| Dry Eye Syndrome | Reflex tearing triggered by surface dryness | Worse in low humidity or air conditioning |
| Blocked Tear Duct | Tears cannot drain, overflow at the inner corner | Watering is constant, not weather-dependent |
| Allergic Conjunctivitis | Histamine response inflames the conjunctiva | Itching, redness, seasonal pattern |
| Eyelid Malposition (Ectropion/Entropion) | Puncta misaligned, can’t collect tears | Visible eyelid turning in or out |
| Wind and Cold Air | Corneal nerves trigger reflex secretion | Only happens outdoors |
| Blepharitis | Inflamed eyelid margins disrupt oil glands | Crusty lids in the morning, gritty feeling |
| Viral Conjunctivitis | Infection activates the immune tear response | Recent cold or pink eye history |
How Blocked Tear Ducts Work Differently
A blocked nasolacrimal duct is a drainage problem, not a production problem. The lacrimal gland is working exactly as intended, but the exit route is partially or fully obstructed. This can happen due to age-related narrowing of the duct, chronic inflammation, nasal polyps, or even a past facial injury. In infants, it’s often a membranous blockage that resolves on its own within the first year of life.
The distinguishing feature is that the tearing tends to be persistent and relatively constant, not triggered by specific environments or activities. You might also notice mucus buildup or a mild sticky discharge at the inner corner of your eye, which is a sign that stagnant tear fluid has become a breeding ground for bacteria. This situation typically requires professional intervention, ranging from irrigation of the duct to a surgical procedure called dacryocystorhinostomy in more severe cases.
Nasolacrimal duct obstruction is estimated to occur in up to 20% of newborns, with the vast majority resolving spontaneously by 12 months. In adults, acquired obstruction becomes more prevalent with age, particularly in women over 50, likely related to anatomical differences in duct diameter and hormonal influences on tissue.
Step-by-Step: How to Identify What’s Causing Your Watery Eyes
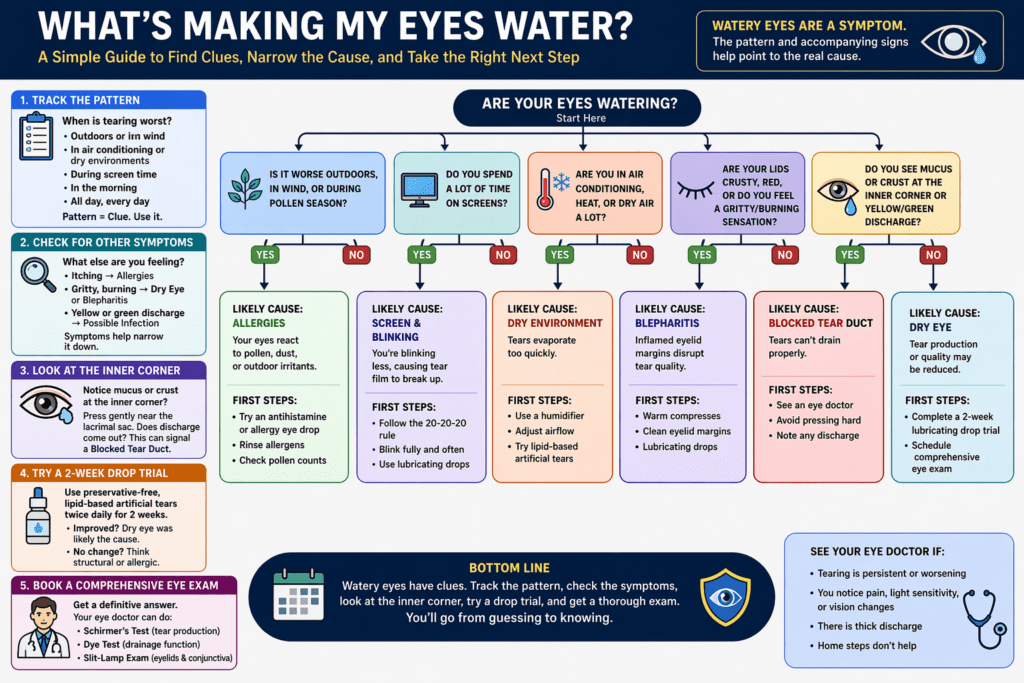
- Track the pattern. Note when tearing is worst — outdoors, in air conditioning, during screen time, in the morning, or consistently all day. Patterns point strongly toward specific causes, such as environmental triggers versus structural drainage problems.
- Check for accompanying symptoms. Itching suggests allergies. A gritty or burning sensation points to dry eye or blepharitis. Yellow or green discharge indicates possible infection. Each combination narrows the diagnosis significantly.
- Examine the inner corner of your eye. If you notice persistent mucus or crustiness specifically at the inner corner (not just at the lash line), this can signal a blocked duct. Gentle pressure near the lacrimal sac that produces discharge is a notable sign.
- Try a structured trial of lubricating drops. Use a preservative-free, lipid-based artificial tear twice daily for two weeks. If tearing significantly improves, dry eye was likely the primary driver. If there’s no change, the cause is probably structural or allergic.
- Book a comprehensive eye exam. A clinician can perform a Schirmer’s test for tear production, dye tests to evaluate drainage function, and slit-lamp examination of your eyelid margins and conjunctiva. This gives a definitive answer that self-assessment cannot.
The Connection Between Eye Coordination and Tear Function
Here’s something few people consider: the way your eyes work together can contribute to surface strain that triggers tearing. When the eyes struggle to coordinate properly, a condition called binocular vision dysfunction, the effort of trying to maintain clear vision places significant strain on the ocular surface. This sustained effort increases blink rate irregularities, disrupts the tear film, and can set off the same reflex tearing cycle associated with dry eye.
Similarly, problems with eye teaming — the ability of both eyes to work as a coordinated pair — can cause one eye to compensate more than the other, leading to uneven tear film distribution across the two eyes. Patients sometimes notice that only one eye waters excessively, which can seem confusing when no obvious structural cause is found in that eye alone.
What Doctors Sometimes Miss: Eyelid Position and Blink Quality
Two factors that are frequently overlooked in a routine exam are eyelid margin position and blink completeness. If the lower eyelid turns slightly outward (ectropion), the punctum moves away from the tear lake and can no longer collect tears effectively. The result is constant overflow, even though the tear duct itself is perfectly clear.
Incomplete blinking, increasingly common among heavy screen users, has been shown to leave the lower third of the cornea chronically exposed and uncoated by the tear film. This localized dryness zone can trigger localized reflex tearing even when overall tear production appears normal on standard tests.
Poor visual alignment and forward head posture can also affect how the eyelids rest against the eye surface, subtly altering the mechanics of tear drainage and blink quality over time. These are the kinds of interconnected factors that a thorough functional eye exam will explore, rather than just measuring visual acuity.
Common Mistakes People Make When Dealing With Watery Eyes
- Using vasoconstrictive “red eye relief” drops repeatedly. These reduce the look of redness but do nothing for the underlying cause, and chronic use can cause rebound inflammation that makes tearing worse.
- Assuming tearing means the eyes are healthy and self-lubricating. Reflex tears don’t substitute for stable basal tear production — the surface is still at risk.
- Rubbing the eyes to clear the watering. Rubbing introduces bacteria, can distort the cornea over time, and further disrupts the tear film structure.
- Treating only the symptom, not the cause. Antihistamines help allergic tearing but will do nothing for a blocked duct. Matching the treatment to the diagnosis is essential.
- Waiting years before seeking care. Chronic epiphora from a blocked duct can lead to recurrent eye infections (dacryocystitis) that are painful and harder to resolve the longer they’re left untreated.
Research into over-the-counter ophthalmic decongestant use suggests that regular use beyond 4 to 5 consecutive days can lead to rebound hyperemia — a worsening redness and irritation cycle that mirrors the rebound effect seen with nasal decongestant sprays. This is a well-documented clinical pattern in eye care practice.
Frequently Asked Questions
Why does my eye water only when I am outside?
Cold air, wind, and bright sunlight all stimulate the trigeminal nerve endings on the corneal surface, which sends a reflex signal to the lacrimal gland to produce more tears. This is a protective response, the eye is trying to flush away the irritant or shield itself from dryness caused by wind evaporating the tear film. Wearing wraparound glasses or sunglasses outdoors significantly reduces this trigger for most people.
Can allergies cause watery eyes even if I don’t sneeze?
Yes, and this is more common than most people realize. Ocular allergies (allergic conjunctivitis) can exist independently of nasal symptoms. The conjunctiva has its own mast cells that release histamine in response to allergens like pollen, pet dander, or dust, causing intense itching and tearing without any sneezing or nasal congestion. If your eyes water in specific seasons or environments and feel itchy, an allergy-focused treatment plan is worth exploring with your eye care provider.
If my eyes are watering, why does the doctor say I have dry eye?
This is the classic paradox of dry eye disease. When your basal tear production is unstable or poor quality, exposed corneal nerve endings trigger a flood of watery reflex tears as an emergency response. These reflex tears overflow immediately because they lack the mucin and lipid components that help tears adhere to the eye. The result is that your eyes water constantly while the underlying surface remains dry and irritated, which is exactly why lubricating drops that address tear quality, not just quantity, are the right treatment.
What is a blocked tear duct, and how do I know if I have one?
The nasolacrimal duct is the channel that carries tears from your eye down into your nasal passage. When it narrows or becomes blocked, tears have nowhere to go except over your lower eyelid. Signs that point to a blocked duct include persistent watering from one eye that doesn’t track with seasonal or environmental patterns, mucus or discharge accumulating at the inner corner of your eye, and occasional swelling or tenderness near the inner corner of your lower eyelid. A simple irrigation test performed by an eye care professional can confirm the diagnosis quickly.
When should I see a doctor for watery eyes?
You should book an appointment if the tearing has lasted more than two to three weeks without an obvious environmental cause, if it’s affecting only one eye, if you notice pain, significant redness, discharge, or light sensitivity alongside the tearing, or if your vision is frequently blurred. Watery eyes that suddenly appear after a head cold or facial trauma also warrant prompt evaluation. While many causes are benign, these specific combinations can signal infections or structural issues that need treatment sooner rather than later.
Conclusion: Your Eyes Are Telling You Something Worth Listening To
Persistent watery eyes are rarely just an inconvenience to tolerate. They’re a signal that something in your tear production, drainage, or ocular surface health needs attention. Whether the cause turns out to be dry eye, a drainage problem, an allergic response, or something more structural, there’s a specific and effective path to relief for each one.
The key is accurate diagnosis, not guessing, not cycling through drugstore drops that don’t address the root cause. Once you know exactly why your eyes are overflowing, treatment becomes straightforward and results can be noticeable within weeks.
If you’ve been living with constantly watery eyes and haven’t found a clear answer, the team at Opto-Mization offers comprehensive functional eye exams that go beyond standard vision checks to examine tear function, eyelid health, drainage, and binocular coordination. You can reach us directly at +1 778-608-5982 to book an assessment and finally get to the bottom of what your eyes have been trying to tell you.
{kind=link}