

Eye pain without visible redness is more common than most people expect, and it often points to internal or neurological causes rather than surface-level irritation. Conditions like dry eye disease, increased eye pressure, optic neuritis, migraines, or binocular vision dysfunction can all produce significant discomfort while leaving the eye looking completely normal from the outside.
You blink. You check the mirror. Nothing looks wrong. No redness, no visible irritation, no foreign object. And yet your eye aches, throbs, or burns in a way that’s hard to ignore. That disconnect between how your eye looks and how it feels is genuinely confusing, and it often leaves people wondering whether something is seriously wrong or whether it will just resolve on its own.
Key Takeaways
- Eye pain without redness is frequently caused by internal conditions like elevated intraocular pressure, dry eye, or optic nerve inflammation rather than surface irritants.
- Binocular vision problems and visual alignment issues can produce chronic eye strain and aching that has no visible external signs.
- Referred pain from migraines, sinus conditions, or even neck tension can manifest directly as eye discomfort.
- Pain behind the eye, pain that worsens with eye movement, or sudden pressure-like pain are all symptoms that warrant prompt professional evaluation.
- Not all eye pain is equal; the location, character, and accompanying symptoms all help distinguish serious causes from benign ones.
- Early assessment by an eye care specialist can prevent minor conditions from progressing into significant vision problems.

What’s Actually Happening When Your Eye Hurts But Looks Fine?
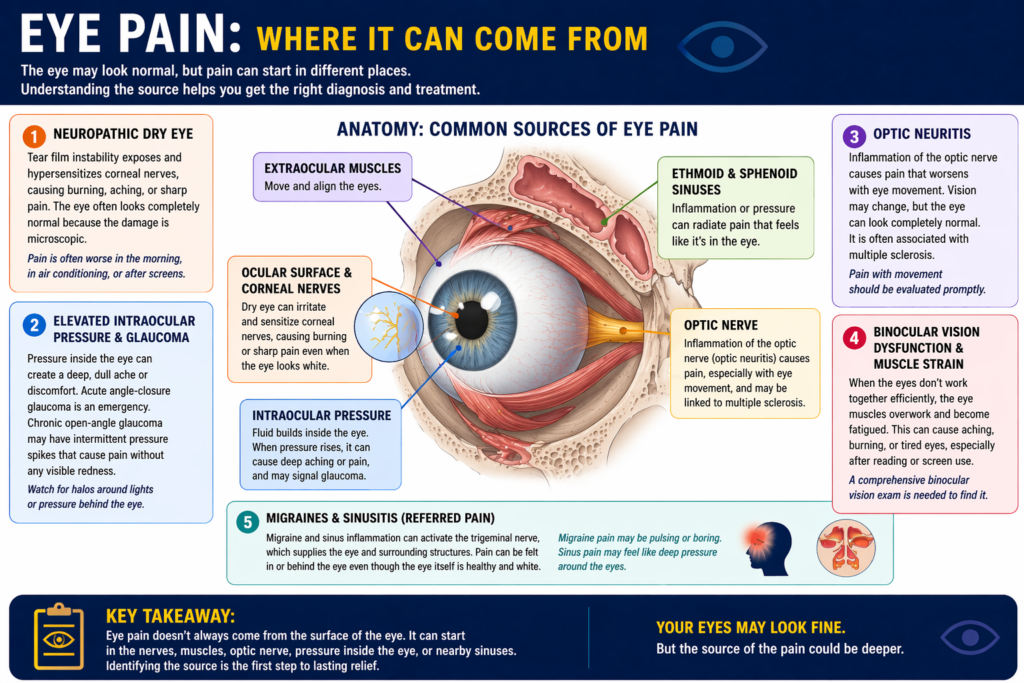
The surface of the eye, the conjunctiva, sclera, and cornea, is where redness originates. When blood vessels in those layers dilate due to irritation, infection, or inflammation, you see that telltale pink or red colour. But pain doesn’t require surface involvement at all. The eye is surrounded by a rich network of sensory nerves, and the structures behind and around it, including the optic nerve, extraocular muscles, intraocular fluid pathways, and adjacent sinuses, can all generate pain signals without touching the visible surface.
Think of it this way: a headache hurts, but your skull doesn’t turn red. The same principle applies here. Pain is a neurological signal, and the eye has many internal pathways capable of producing it independently of any surface change.
The Most Common Causes of Eye Pain Without Redness
Dry Eye Disease (Moderate to Severe Stages)
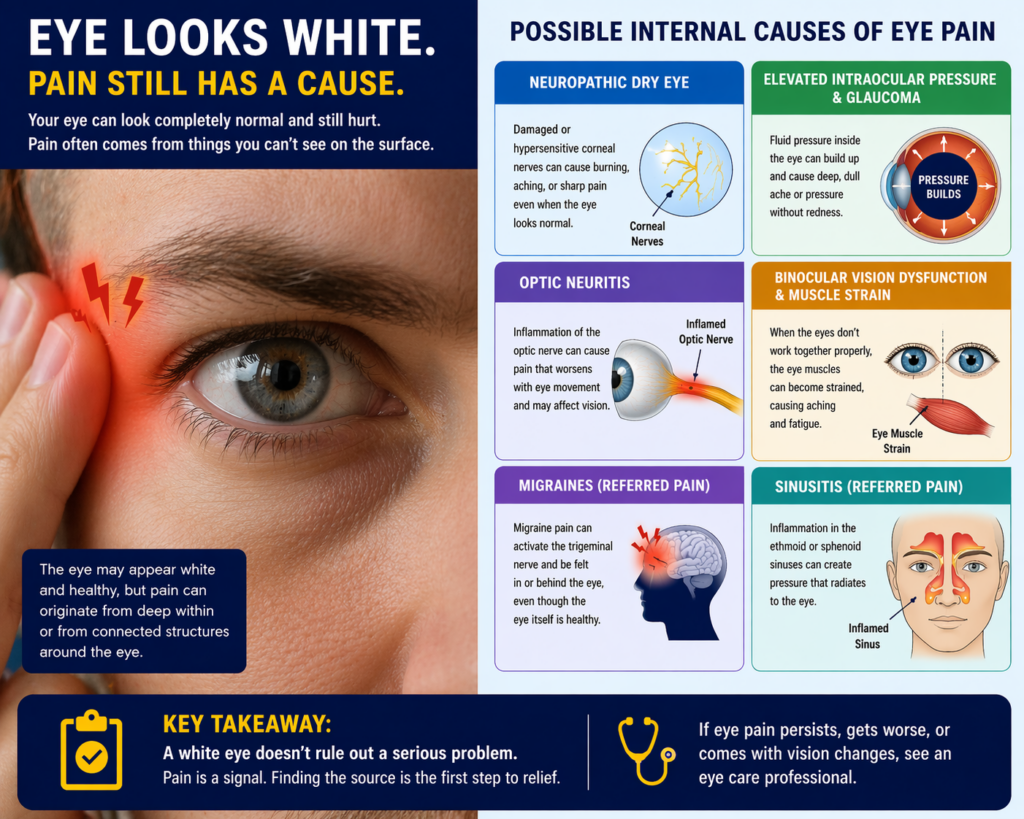
Dry eye disease affects an estimated 16 million adults in the United States alone, and in its more advanced stages it frequently produces burning, aching, or sharp discomfort without significant visible redness. As the tear film becomes increasingly unstable, corneal nerve endings become exposed and hypersensitized, a condition known as corneal neuropathy, which can cause disproportionately intense pain relative to what the eye looks like externally.
Many patients with neuropathic dry eye report that their pain is worst in the morning, in air-conditioned spaces, or after prolonged screen use. The eye may appear entirely white because the inflammatory response is occurring at a microscopic level, below what the naked eye can detect.
Elevated Intraocular Pressure and Glaucoma
Acute angle-closure glaucoma is one of the few genuine ophthalmic emergencies, and it classically presents as severe eye pain, nausea, and blurred vision, often without the dramatic redness that most people associate with serious eye conditions. Chronic open-angle glaucoma, the far more common form accounting for roughly 90% of glaucoma cases, typically causes no pain at all in its early stages, but intermittent pressure spikes can generate dull orbital aching that patients frequently misattribute to tension headaches.
If the pain feels like pressure from behind the eye or is accompanied by mild halos around lights, getting intraocular pressure measured is a reasonable and important first step.
Optic Neuritis
Optic neuritis is inflammation of the optic nerve, and pain with eye movement is its most recognizable feature. The discomfort typically sits behind the eye and intensifies when the eye moves side to side or up and down. The eye itself may appear completely normal to anyone looking at it from the outside, because the inflammation is happening along the nerve rather than on the ocular surface.
Optic neuritis has a known association with multiple sclerosis; approximately 50% of people with MS will experience at least one episode of optic neuritis during their lifetime, and in many cases it is the initial presenting symptom of the condition. Because of this association, any case of pain with eye movement that comes with vision changes should be evaluated promptly by a neurologist or neuro-ophthalmologist.
Binocular Vision Dysfunction and Eye Muscle Strain
When the two eyes don’t work together efficiently, the extraocular muscles responsible for coordination are forced to compensate continuously. That sustained muscular effort produces a very real aching, burning, or tired feeling in and around the eye. Problems with eye teaming are particularly common in people who spend long hours reading, using screens, or doing close-up detailed work.
What makes this cause easy to overlook is that the discomfort often feels like a generalized eye fatigue rather than a sharp pain, and the eyes look completely normal. A comprehensive binocular vision assessment, not just a standard acuity test, is needed to identify it.
Referred Pain From Migraines and Sinusitis
Migraine headaches are notorious for concentrating pain around and behind the eye. The trigeminal nerve, which supplies sensation to much of the face including the eye socket, is heavily involved in migraine pain pathways. Patients often describe the sensation as a boring or pulsing pain directly in or behind the eye, and it can occur with or without the classic throbbing head pain.
Similarly, ethmoid and sphenoid sinus inflammation sits in very close anatomical proximity to the eye socket. Pressure or infection in those sinuses can radiate pain that feels unmistakably like it originates in the eye itself, and the sclera may remain perfectly white throughout.
How Visual Alignment Issues Play a Bigger Role Than Most People Realize
Chronic, unexplained eye aching that comes and goes without any visible sign is one of the more underappreciated presentations of visual alignment problems. When the visual system is working against itself to maintain clear, single binocular vision, the strain accumulates over hours of near work and manifests as eye pain, frontal headaches, and sometimes neck or shoulder tension.
These symptoms often get attributed to screen time, stress, or needing a stronger glasses prescription, when in fact the underlying issue is a subtle misalignment that requires a specific type of assessment and intervention to identify.
Understanding the Difference: Surface Pain vs. Deep Pain
| Pain Type | Typical Sensation | Likely Origin | Visible Redness? |
| Surface / Ocular | Gritty, scratchy, burning | Cornea, conjunctiva | Usually yes |
| Orbital / Deep | Aching, pressure, throbbing | Optic nerve, sinuses, muscles | Often no |
| Neuralgia | Sharp, shooting, stabbing | Trigeminal nerve branches | No |
| Muscle Strain | Tired, dull ache, fatigue | Extraocular muscles | No |
| Referred Pain | Radiating, pulsing | Migraine, sinus, cervical | No |
When Should Eye Pain Without Redness Concern You?
Not every episode of eye discomfort demands an emergency visit. But certain patterns do warrant getting an evaluation sooner rather than later. Knowing which signals to watch for helps you make that call with confidence rather than guessing.
- Pain that worsens with eye movement is a classic sign of optic neuritis and should be evaluated promptly, especially if paired with any change in colour vision or visual clarity.
- Sudden, severe pressure behind one eye with nausea or halos around lights may indicate acute angle-closure glaucoma, a genuine emergency that requires same-day care.
- Pain consistently worse in the morning that eases throughout the day often suggests elevated intraocular pressure during sleep, a pattern worth discussing with an eye care provider.
- Persistent aching that correlates with reading or screen use and improves with rest points toward a binocular vision or vergence-related cause.
- Any vision changes accompanying the pain, including blurring, double vision, or dimming, always raise the priority level.
Step-by-Step: What to Do When Your Eye Hurts But Looks Normal
- Characterize the pain honestly. Note whether it’s a surface sensation (gritty, scratchy) or a deeper ache or pressure. This distinction is genuinely useful information for your eye care provider.
- Track the pattern. Does it correlate with screen use, certain lighting, reading, or time of day? Patterns like “worse after an hour of reading” or “every morning when I wake up” carry real diagnostic weight.
- Note accompanying symptoms. Any nausea, halos, vision changes, or pain that intensifies with eye movement should be recorded and communicated clearly.
- Avoid self-diagnosing with over-the-counter drops. Vasoconstrictor redness-relief drops in particular can mask symptoms and, with repeated use, cause rebound inflammation that complicates the picture further.
- Book a comprehensive eye exam, not just a standard vision test. Ask specifically about binocular vision evaluation and intraocular pressure measurement, as these are not automatically included in every routine checkup.
- Share your full history. Mention headaches, neck pain, sinus issues, and any neurological conditions, even if they seem unrelated. Pain around the eye rarely exists in complete isolation from the rest of the body.
A Note on Aging and Changing Tear Chemistry
Hormonal shifts associated with aging, particularly the decline of androgens after age 40, directly reduce the lipid layer of the tear film. This creates the conditions for chronic dry eye and corneal nerve sensitization even in people who have never experienced eye problems before. Options like presbyopia eye drops and newer prescription tear treatments have changed how this population can be managed, but the underlying pain mechanism is often neurological rather than purely inflammatory.
Common Mistakes People Make With Unexplained Eye Pain
- Assuming no redness means no problem, and delaying evaluation until symptoms worsen significantly.
- Using over-the-counter redness-relief drops, which address surface vessel dilation but do nothing for internal or neurological causes of pain.
- Attributing all eye discomfort to screen time and stopping there, without investigating whether a binocular vision issue is the actual driver.
- Treating only the headache without ever addressing the eye component, especially in migraine patients who may have an undiagnosed visual trigger.
- Skipping the intraocular pressure check during routine exams, particularly if there’s a family history of glaucoma.
- Assuming the pain will resolve on its own without any lifestyle or optical intervention, leading to months of unnecessary discomfort.
Frequently Asked Questions
Why does my eye hurt but I don’t see anything in it?
When there’s no visible foreign body and no redness, the pain is typically originating from inside or around the eye rather than on its surface. Internal causes like elevated eye pressure, optic nerve inflammation, or binocular muscle strain all produce real, sometimes intense discomfort without leaving any visible external sign. A comprehensive eye exam is the most reliable way to identify what’s actually causing the pain.
What are common causes of eye pain?
The most common causes include dry eye disease, elevated intraocular pressure, binocular vision dysfunction, optic neuritis, migraines, and referred pain from sinus conditions or cervical tension. Surface-level causes like corneal abrasions or conjunctivitis tend to produce visible redness, while internal and neurological causes frequently do not. The character and location of the pain, along with any accompanying symptoms, help differentiate between them.
What is a red flag for eye pain?
Several patterns warrant urgent attention: sudden severe pain with nausea or halos around lights (possible acute glaucoma), pain that worsens noticeably when you move your eye (possible optic neuritis), any pain accompanied by sudden vision loss or double vision, and pain following eye trauma. These situations benefit from same-day or emergency evaluation rather than a wait-and-see approach. When in doubt, it’s always safer to have it assessed quickly.
What causes pain in only one eye?
Unilateral eye pain often points to a localized cause in that specific eye or orbit, such as elevated pressure in one eye, early optic neuritis on that side, a corneal issue invisible to the naked eye, or cluster headaches, which are characterized by severe, focused pain around one eye. Migraine can also concentrate pain unilaterally. If the pain in one eye is new, persistent, and differs from anything you’ve experienced before, an evaluation is a reasonable next step.
Can eye pain go away on its own?
It depends entirely on the cause. Eye strain from prolonged screen time or a mild binocular vision issue often resolves with rest, breaks, or corrective lenses. Pain from dry eye can fluctuate significantly. However, pain from elevated intraocular pressure or optic neuritis will not resolve without treatment and can lead to permanent damage if left unaddressed. The challenge is that it’s very difficult to know which category you’re in without a professional assessment, so persistent or worsening pain should not be left to resolve on its own.
Final Thoughts: Your Eye Doesn’t Have to Look Sick to Need Attention
The absence of redness is not a reassurance that everything is fine. Some of the most clinically important causes of eye pain produce no visible changes whatsoever, which is exactly what makes them easy to dismiss and easy to miss. Understanding that pain is a neurological signal, not just a surface phenomenon, changes how you interpret what your eye is trying to tell you.
If you’ve been experiencing unexplained eye discomfort, dull orbital aching, pain with eye movement, or chronic eye fatigue that rest doesn’t fully resolve, a proper evaluation goes well beyond checking whether you need new glasses. A thorough assessment of binocular function, intraocular pressure, tear film quality, and optic nerve health gives you a real picture of what’s happening.
Ready to Find the Actual Cause of Your Eye Pain?
At Opto-Mization, our team specializes in the kind of detailed functional vision assessments that go beyond standard testing to uncover what’s really driving your discomfort. Whether it’s a binocular vision issue, pressure-related pain, or something else entirely, you deserve answers, not guesswork.
Call us at +1 778-608-5982 to schedule a comprehensive evaluation. Your eyes shouldn’t hurt, and with the right assessment, they don’t have to.
{kind=link}